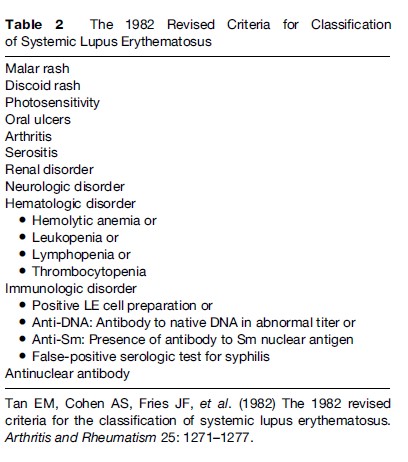
It has long been known that aberrant reaction to sunlight is present in almost all patients with a cutaneous or systemic manifestation of LE. Therefore, photosensitivity is listed as one of the American College of Rheumatology (ACR) criteria for the classification of SLE, although it is poorly defined as ‘‘a result of an unusual reaction to sunlight by patient history or physician observation’’ (Tan et al., 1982: 1274).Therefore, a detailed clinical history is important for the diagnosis and assessment of photosensitivity in patients with LE, including several key components, such as the morphology of the rash, duration, distribution, and the relationship to sun exposure and specific symptoms (e.g., pain, pruritus, burning, blistering, and swelling). Each of these symptoms may provide clues to the nature of the photosensitive eruption and, thus, the diagnosis. In addition, photoprovocation tests with long-wave UV light (UVA) and sunburn UV light (UVB) irradiation have been found to be an objective way to evaluate photosensitivity in patients with CLE. A standardized protocol for phototesting has been developed and optimized by taking into account multiple factors, such as light source, test area of irradiated skin, dose of UV exposure, and frequency of irradiation. In 2001, photoprovocation test reactions were evaluated in more than 400 patients with different subtypes of CLE and most of the patients developed characteristic skin lesions using combined UVA and UVB. Altogether, skin lesions were observed in 54% of patients with LE; 42% of these patients reacted to UVB irradiation only and 34% to UVA irradiation only. Interestingly, there were substantial differences in the clinical subtypes of LE with regard to response to the different UV wavelength. Patients with ICLE have been found to be the most photosensitive subtype, as phototesting revealed characteristic skin lesions in 72% of these patients. In contrast, pathologic skin reactions were induced by UV irradiation in 63% of patients with SCLE, in 60% of patients with ACLE, and in 45% of patients with CCLE. Moreover, photoprovocation tests are also helpful for the education of patients on protective measures. It has been demonstrated that broadband sunscreens can suppress the induction of skin lesions by UV irradiation in patients with CLE. Therefore, consequent protection against UV light as well as other physical and mechanical injuries may be of significant value for the course and prognosis of both CLE and SLE (Table 2).