Some potentially malignant (precancerous) clinical lesions that can progress to OSCC include especially:
- Erythroplasia (erythroplakia): The most likely lesion to progress to severe dysplasia or carcinoma. Erythroplastic lesions are velvety red plaques, which in at least 85% of cases show frank malignancy or severe dysplasia. Carcinomas are seen 17 times more frequently in erythroplakia than in leukoplakia (but leukoplakias are far more common).
- Leukoplakia, particularly where admixed with red lesions, as in speckled leukoplakia, and proliferative verrucous leukoplakia, sublingual leukoplakia, candidal leukoplakia, syphilitic leukoplakia (now exceptionally rare).
- Lichen planus.
- Oral submucous fibrosis ( Jeng et al., 2001).
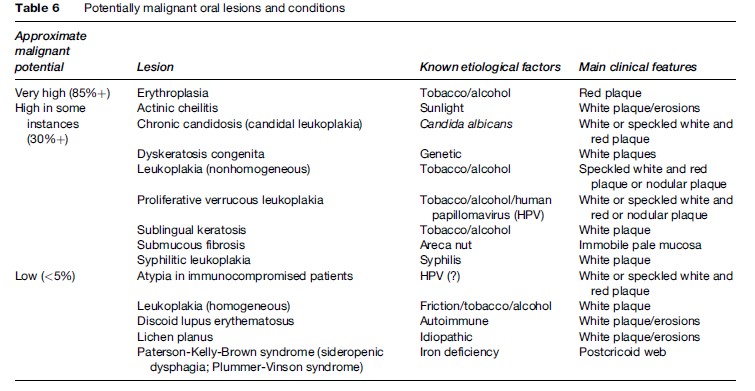
Apart from these lesions, most other potentially malignant lesions or conditions have only a very low incidence of dysplasia or malignant change (Table 6).
There is a highly significant increase in the incidence of OSCC of the tongue in systemic sclerosis (Derk et al., 2005) and an increase of OSCC in transplant recipients (Scheifele et al., 2005).
Prevention Of Oral Cancer
There is remarkably little good-quality evidence on the prevention of OSCC. However, OSCC shares several risk factors with other diseases, and is thus potentially amenable to prevention using the principles of the Common Risk Factor Approach (Sheiham and Watt, 2000). Health promotion campaigns centered on cessation of tobacco use in particular have been advocated and directed either at primary prevention or at preventing the malignant transformation of potentially malignant lesions and conditions. Most notably, Warnakulasuriya et al. (1991) used primary health-care workers in Sri Lanka not only to screen for oral cancer and precancer, but also to deliver tobacco cessation advice to high-risk subjects.
However, despite a reduction in tobacco product consumption in many developed countries, oral cancer incidence and mortality has not always fallen in these countries, leading some researchers to hypothesize that alcohol consumption (Hindle et al., 2000), genetic factors, and environmental factors such as infective agents (Scully et al., 2005) are increasing in relative importance.
Chemopreventive clinical trials aim to prevent the potentially malignant lesions or attempt to prevent malignant transformation or aim to cause regression of lesions in high-risk patient groups (Zaridze et al., 1993; Mathew et al., 1995).